The Therapeutic Gap in Covid-19
Mon Oct 18 2021
The therapeutic gap in COVID-19
Passive immunity shows a beneficial effect in the earliest stage of COVID-19 infection, prior to onset of symptoms, while immunosuppressants are beneficial for patients with critical respiratory failure much later in the course of infection. Therefore, a therapeutic gap exists and must be filled if the infection is not detected early and disease escalation is to be prevented.
Introduction
By October 2021, more than 4.8 million deaths were associated with coronavirus disease 2019 (COVID-19) worldwide (https://coronavirus.jhu.edu/). Despite the development of vaccines preventing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, COVID-19 drug development remains a top priority due to the threat of new vaccine-resistant variants. Several drug molecules with different mechanisms of action are currently being clinically tested against COVID-19. In light of the pathogenesis of COVID-19, it is evident that the appropriateness of any treatment depends on the stage of the disease. Furthermore, we need to identify which kinds of drugs will be necessary to combat future SARS-CoV-2 variants.
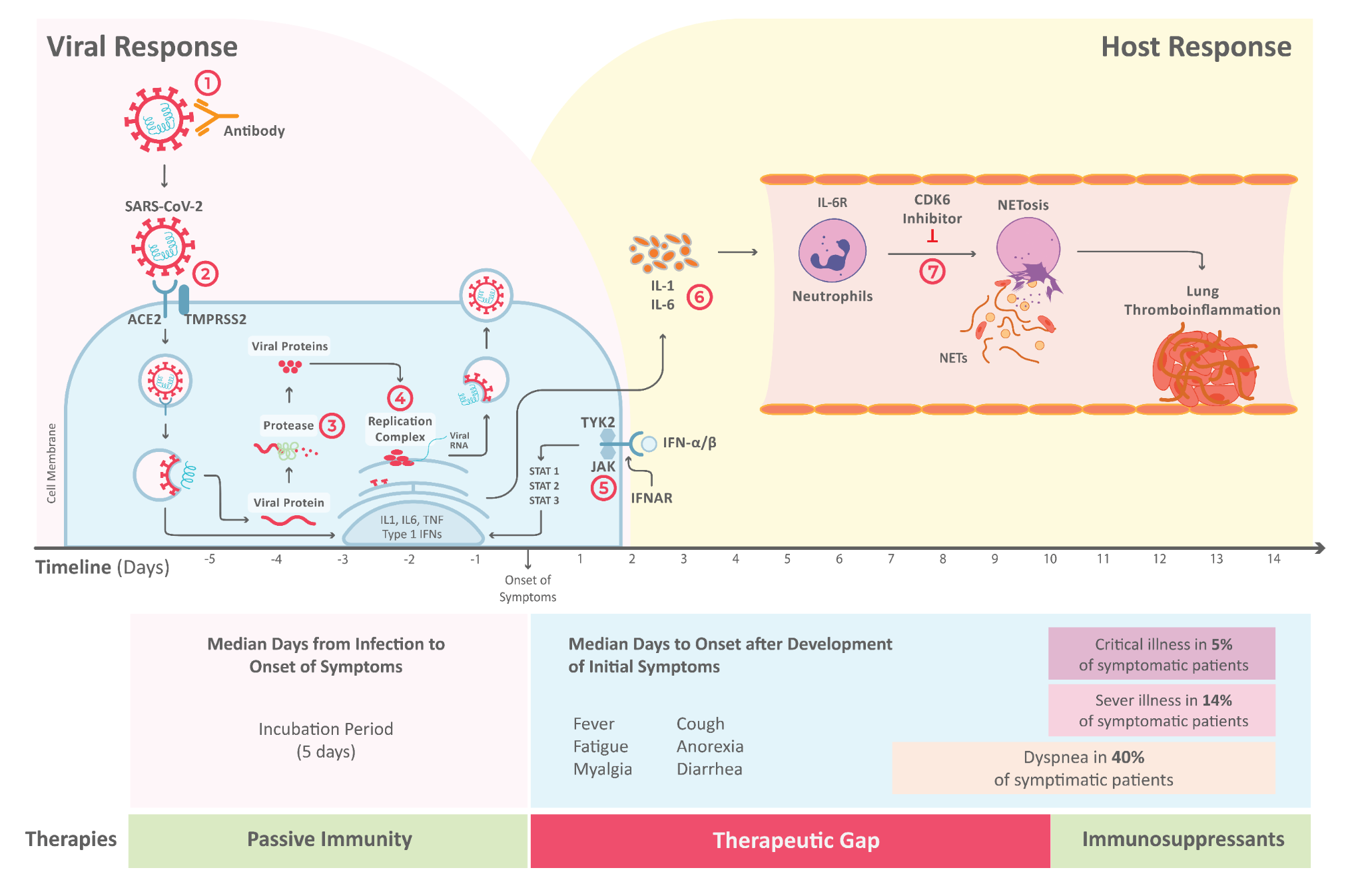
Fig. 1. The life cycle of SARS-CoV-2 and the corresponding pathogenesis of COVID-19 with the seven identified drug mechanisms: ① Passive immunity; ② Entry inhibitors; ③ Protease inhibitors; ④ Polymerase inhibitors; ⑤ JAK inhibitors; ⑥ Immunosuppressants; ⑦ NETosis inhibitors.
The life cycle of SARS-CoV-2 and the corresponding pathogenesis of COVID-19 display two phases: a viral response and a host-response phase (Fig. 1). In the viral response phase, the virus enters the host cell and viral replication begins. Approximately five days after infection and successful replication, initial mild and moderate symptoms such as fever, cough, fatigue, anorexia, myalgia, and diarrhea are observed in conjunction with a decrease in lymphocyte cell count (lymphopenia). The following host-response phase determines the severity of the disease: in some patients, uncontrolled overreaction of the immune system – so-called virus-induced immunopathology – requires hospitalization and respiratory support due to acute respiratory distress syndrome (ARDS).(1) Thus, severe cases of COVID-19 originate from an immune overreaction rather than from the viral infection itself.
Corresponding to the two stages of COVID-19 pathogenesis, drugs can be divided into antivirals and immuno-modulators (Tab. 1). Antiviral drugs target crucial points in the viral life cycle, while immuno-modulators aim to adjust the host immune response.
Tab. 1. Overview of the seven drug classes that are being clinically tested against COVID-19. Passive immunity ① through monoclonal antibodies shows effect at the beginning of the infection, while immunosuppressants ⑥ are beneficial for the treatment of the later immune overreaction. Therefore, a therapeutic gap exists if the infection is not detected early and a possible immune overreaction is to be prevented.
| No. | Mechanism | Disease stage | Drug | Clinical evidence | |
| Antiviral | ① | passive immunization | directly after exposure | casirivimab/ imdevimab, bamlanivimab/ etesevimab, sotrovimab | yes(3) |
| ② | entry inhibitor | viral response phase | hydroxychloroquine, chloroquine | no(4) | |
| ③ | protease inhibitor | viral response phase | lopinavir/ritonavir | no(4,5) | |
| ④ | polymerase inhibitor | viral response phase | favipiravir, remdesivir, molnupiravir, ivermectin | no(4,6,8,9,17) | |
| Immuno-Modulator | ⑤ | JAK inhibitor | moderate / severe to prevent & treat thrombo- inflammation | baricitinib, ruxolitinib | no(11),(12) |
| ⑥ | immuno- suppressants | severe / critically ill to treat thrombo- inflammation | dexamethasone, sarimulab, tocilizumab, colchicine | yes (dexamethasone, sarimulab, tocilizumab) (13,14); no (colchicine)(15) | |
| ⑦ | NETosis inhibitor | moderate / severe to prevent thrombo- inflammation | abemaciclib, palbociclib, ribociclib | not yet tested |
Antivirals
① Passive immunity
Analogous to a vaccination, passive immunity describes a short-term immunization achieved by direct administration of antibodies against the spike protein of SARS-CoV-2, a key mediator of viral infectivity essential for entering the host cell.(2) The Food and Drug Administration (FDA) issued an emergency use authorization for the monoclonal antibodies casirivimab/imdevimab, bamlanivimab/etesevimab, and sotrovimab.(3) Nonetheless, monoclonal antibodies are expensive and difficult to handle because they require a cold chain. More importantly, passive immunity is only effective when the antibodies are administered very soon after exposure to the virus – administration after occurence of first symptoms is too late.
② Entry inhibitors
Entry inhibitors prevent a virus from entering a cell by blocking receptors on the host cell. The SARS-CoV-2 spike protein engages angiotensin-converting enzyme 2 (ACE2) as the entry receptor and employs the cellular serine protease TMPRSS2 for spike protein priming.(2) As hydroxychloroquine, a malaria treatment, had been reported to bind to the ACE2 receptor, it received emergency use authorization by the FDA from April to June 2020. The authorization was withdrawn when further clinical investigations showed that hydroxychloroquine and its derivative chloroquine are not effective for preventing infection.(4)
③ Protease inhibitors
Following entry, the viral RNA is released and translated to the polyproteins pp1a and pp1ab that are further processed by viral cysteine proteases, papain-like protease (PLpro) and 3C-like protease (3CLpro), into the individual non-structural proteins that form the viral replication and transcription complex (RTC).(2) The protease inhibitor lopinavir-ritonavir showed in vitro activity against SARS-CoV-2; however, clinical investigations revealed that lopinavir-ritonavir did not reduce 28-day mortality of hospitalized COVID-19 patients.(5) Protease inhibitors designed directly for the viral cysteine proteases such as Pfizer’s PF-07321332 are still in development (ClinicalTrials.gov Identifier: NCT04960202).
④ Polymerase inhibitors
The RNA-dependent RNA-polymerase (RdRP) is a crucial enzyme in the virus life cycle both for replication and transcription and has thus been suggested as a promising drug target.(2) Previously reported inhibitors of the RdRP such as favipiravir, remdesivir, and molnupiravir have been clinically tested against COVID-19. While favipiravir and remdesivir showed promise in initial studies, further clinical investigations revealed no clinical effects.(4,6) Molnupiravir showed recently strong effects to prevent deaths.(7) Nonetheless, the Drug Controller General of India denied that molnupiravir has an effect.(8) In addition, it has been claimed that ivermectin, an antiparasitic agent, binds to the RCT, thereby inhibiting viral replication in vitro. However, a large randomized clinical trial showed that ivermectin has no effect.(9)
Immuno-modulators
⑤ JAK inhibitors
Severe and critically ill disease courses in COVID-19 are caused by an overreaction of the immune system. It is postulated that mitigating the immune response and preventing a hyperinflammatory state may improve clinical outcomes.(1) Baricitinib, an orally administered selective inhibitor of Janus kinase (JAK) 1 and 2, is a mild immunosuppressant inhibiting the intracellular signalling pathway of cytokines known to be elevated in severe COVID-19, including interleukin 6 (Fig. 1). It also acts against SARS-CoV-2 through the impairment of AP2-associated protein kinase 1 and the prevention of SARS-CoV-2 cellular entry. In combination with remdesivir, baricitinib improved outcomes in a randomized controlled trial of hospitalized COVID-19 patients. However, the effects of baricitinib and its derivative ruxolitinib did not reach statistical significance compared to a control group that was treated with the immunosuppressant dexamethasone.(10,11,12)
⑥ Immunosuppressants
Immunosuppressants such as dexamethasone or interleukin 6 receptor (IL-6R) antagonists tocilizumab and sarilumab have been successfully tested to block the immune system’s overreaction in the form of a cytokine storm in critically ill COVID-19 patients.(13,14) However, there is a trend indicating that although treatment with corticosteroid dexamethasone is beneficial among patients with critical respiratory failure, it is nonetheless harmful in patients without respiratory failure. Notably, mild immunosuppressants such as colchicine have shown no effect on critically ill COVID-19 patients.(15)
⑦ NETosis inhibitors
Critically ill COVID-19 status is characterized by infiltration of the lungs with macrophages and neutrophils that cause diffuse lung alveolar damage, the histological equivalent to ARDS. Neutrophils are an important component of the host defense response against invading pathogens and develop so-called neutrophil extracellular traps (NETs), web-like structures of nucleic acids wrapped with histones that detain viral particles, through NETosis, a regulated form of neutrophil cell death. However, ineffective clearance and dysregulation of NETosis result in pathological effects such as thromboinflammation as described above. Cyclin-dependent kinases (CDK) 4 and 6 have been previously described as regulators of NETosis. Inhibition of CDK4/6 blocks NETs formation in a dose-responsive manner but does not impair oxidative burst, phagocytosis, or degranulation.(1) This indicates that CDK4/6 inhibition specifically affects NET production rather than universally modulating inflammatory pathways (in contrast to IL-6 inhibitors). This is supported by Grinshpun et al.’s report that COVID-19 progression was halted for a breast cancer patient on CDK4/6 inhibitor therapy. Once the drug was withdrawn, the full classic spectrum of illness appeared, including oxygen desaturation necessitating a prolonged hospital stay for close monitoring of the need for invasive ventilations.(16) Selective inhibition of NETosis is a particularly attractive treatment because CDK6 inhibitors can prevent the cytokine storm and, thus, later intensive care.(1)
Outlook
In summary, seven drug classes, each with different mechanisms of action, have been identified for the treatment of COVID-19. However, clinically relevant effects were only confirmed for two of these classes (Tab. 1). Passive immunity through monoclonal antibodies shows an effect at the beginning of the infection, while immunosuppressants are beneficial for the treatment of the later immune overreaction. Therefore, a therapeutic gap exists if the infection is not detected early and a possible immune overreaction is to be prevented. The immune overreaction and, from there, intensive care must be circumvented in order to avoid overwhelming the health care system and triggering lockdowns in the event of further waves. This gap urgently needs to be closed in order to be prepared for any future variants able to evade vaccine protection.
In particular, CDK6 inhibitors represent a swift solution to this problem, as they have already been approved for the treatment of breast cancer. In the case reported by Grinshpun et al., the CDK6 inhibitor was administered prior to infection, therefore it was not harmful in the early course of the disease (like immunosuppressants), but protected against thromboinflammation and thus prevented the necessity of intensive care. Another advantage rendering CDK6 an attractive drug target is that since it is a human protein, mutations of the virus do not influence drug action - in stark contrast to antivirals. Ultimately, CDK6 inhibitors might become so-called magic bullets, as they could be used against all virus-induced immune pathologies, and thus also contain future pandemics of novel viruses. Further clinical investigations will show whether this hope is justified.
References
1. Klinger J, Ravarani C, Bannard C, Lamparter M, Schwinges A, Cope J, Baukmann H, Schmidt M. Critically ill COVID-19 status associated trait genetics reveals CDK6 inhibitors as potential treatment. doi:10.21203/rs.3.rs-568366/v1
2. V’kovski P, Kratzel A, Steiner S, Stalder H, Thiel V. Coronavirus biology and replication: implications for SARS-CoV-2. Nat Rev Microbiol (2021) 19:155–170.
3. Taylor PC, Adams AC, Hufford MM, de la Torre I, Winthrop K, Gottlieb RL. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat Rev Immunol (2021) 21:382–393.
4. WHO Solidarity Trial Consortium, Pan H, Peto R, Henao-Restrepo A-M, Preziosi M-P, Sathiyamoorthy V, Abdool Karim Q, Alejandria MM, Hernández García C, Kieny M-P, et al. Repurposed Antiviral Drugs for Covid-19 - Interim WHO Solidarity Trial Results. N Engl J Med (2021) 384:497–511.
5. Horby PW, Mafham M, Bell JL, Linsell L, Staplin N, Emberson J, Palfreeman A, Raw J, Elmahi E, Prudon B, et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet (2020) 396:1345–1352.
6. Hassanipour S, Arab-Zozani M, Amani B, Heidarzad F, Fathalipour M, Martinez-de-Hoyo R. The efficacy and safety of Favipiravir in treatment of COVID-19: a systematic review and meta-analysis of clinical trials. Sci Rep (2021) 11:11022.
7. Willyard C. How antiviral pill molnupiravir shot ahead in the COVID drug hunt. Nature (2021) doi:10.1038/d41586-021-02783-1
8. Merck drug less effective against moderate COVID -India regulatory source. Reuters (2021) Available at: https://www.reuters.com/business/healthcare-pharmaceuticals/merck-drug-less-effective-against-moderate-covid-india-regulatory-source-2021-10-08/ [Accessed October 14, 2021]
9. López-Medina E, López P, Hurtado IC, Dávalos DM, Ramirez O, Martínez E, Díazgranados JA, Oñate JM, Chavarriaga H, Herrera S, et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial. JAMA (2021) 325:1426–1435.
10. Kalil AC, Patterson TF, Mehta AK, Tomashek KM, Wolfe CR, Ghazaryan V, Marconi VC, Ruiz-Palacios GM, Hsieh L, Kline S, et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Engl J Med (2021) 384:795–807.
11. Marconi VC, Ramanan AV, de Bono S, Kartman CE, Krishnan V, Liao R, Piruzeli MLB, Goldman JD, Alatorre-Alexander J, de Cassia Pellegrini R, et al. Baricitinib plus Standard of Care for Hospitalized Adults with COVID-19. medRxiv (2021) Available at: https://www.medrxiv.org/content/10.1101/2021.04.30.21255934v1.full-text
12. Novartis provides update on RUXCOVID study of ruxolitinib for hospitalized patients with COVID-19. Available at: https://www.novartis.com/news/media-releases/novartis-provides-update-ruxcovid-study-ruxolitinib-hospitalized-patients-covid-19 [Accessed July 28, 2021]
13. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, Staplin N, Brightling C, Ustianowski A, et al. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med (2021) 384:693–704.
14. REMAP-CAP Investigators, Gordon AC, Mouncey PR, Al-Beidh F, Rowan KM, Nichol AD, Arabi YM, Annane D, Beane A, van Bentum-Puijk W, et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with Covid-19. N Engl J Med (2021) doi:10.1056/NEJMoa2100433
15. Group RC, RECOVERY Collaborative Group, Horby PW, Campbell M, Spata E, Emberson JR, Staplin N, Pessoa-Amorim G, Peto L, Wiselka M, et al. Colchicine in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. doi:10.1101/2021.05.18.21257267
16. Grinshpun A, Merlet I, Fruchtman H, Nachman D. A Protracted Course of COVID19 Infection in a Metastatic Breast Cancer Patient During CDK4/6 Inhibitor Therapy. Front Oncol (2020) 10:1085.
17. Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, Hohmann E, Chu HY, Luetkemeyer A, Kline S, et al. Remdesivir for the treatment of Covid-19 - final report. N Engl J Med (2020) 383:1813–1826.
